
Skin incision
MAKING THE INCISION:
GOAL: Incise the skin completely for the desired distance with a scalpel blade
- What direction do you want to make the incision?
The right handed surgeon usually stands on the right side of the patient and makes the incision from left to right. The left handed surgeon typically stands on the left side of the patient and makes the incision from left to right.
The fingertip grip allows more blade to contact the tissues and better cushioning against sudden changes in pressure or direction.
The belly of the blade as it has the longest cutting surface. Using this part of the blade is especially important when making long incisions.
Slide cutting is the most efficient for long incisions. Remember to keep the blade perpendicular to the surface and stretch the skin laterally with the non-dominant hand as the incision is being made. The pressure on the blade is adjusted so the skin is incised completely in a single pass. Insufficient pressure on the blade causes a tentative incision that needs multiple attempts to complete and creates jagged edges. Too much pressure also cuts into the deeper tissue layers.
Subcutaneous incision
- subcutaneous tissue is composed of loose connective tissue with variable amounts of fat
- is closely connected to overlying skin and underlying abdominal wall
Goals:
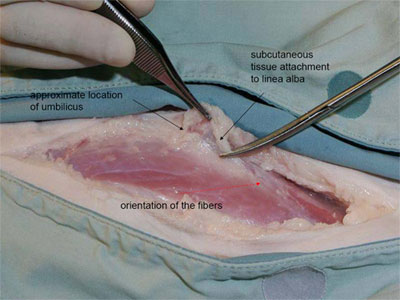
- incise subcutaneous tissue between skin and underlying abdominal wall just enough to accurately identify the linea alba
- linea alba can be difficult to identify
- helpful landmarks:
- umbilicus (the linea is wider and easier to identify at this point)
- orientation of fascia and muscle fibers (the fibers angle caudomedially and join at the linea
- subcutaneous fascia attaches to edges of linea alba
- helpful landmarks:

Methods of subcutaneous incision
-
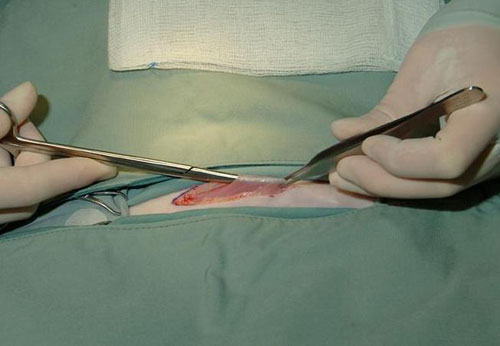
Detach subcutaneous tissue (SQ) from the linea alba
- small cut is made in SQ tissue
- one blade of the scissors is placed into the cut while other arm remains visible
- use push cutting technique to advance the scissors
- cleanly separates SQ off the linea alba
- technique is very good for isolating the linea alba but creates a lot of dead space that then must be closed
- once skill at identifying linea alba is developed, it will seldom be necessary
-
Blunt dissection
- used to determine approximate location of the linea when unsure of location
- once skill at identifying the linea is developed, it will seldom be necessary
- Avoid excessive blunt dissection
- creates excess dead space for fluid to accumulate in the recovery period (ie. seroma).
- Avoid excessive blunt dissection
-
Scalpel blade incision
- scalpel blade is used to sharply incise SQ tissue directly over the linea alba
- BEST after become skilled at identifying linea alba
- causes the least tissue trauma
- creates minimal dead space
-
Modifications for laparotomies in male dogs
- Prepuce is retracted to opposite side of proposed incision and secured with towel clamp
TECHNIQUE
- Incision begins on ventral midline, but as prepuce is approached, it curves along base of prepuce closest to surgeon (usually right side)
- preputial muscles are divided with subcutaneous tissues between umbilicus and prepuce
- are distinct developments of cutaneous trunci muscle
- located adjacent to ventral midline in area of the umbilicus and extend caudally to the prepuce
- called preputial muscles, but look more like tendons
- during closure, must differentiate them from rectus fascia or linea alba
- need to be closed or prepuce may be malpositioned
- preputial branch of caudal superficial epigastric vessels are identified and ligated before incising subcutaneous tissue in cranial preputial area
- Retract the skin and subcutaneous tissues laterally towards side of the clamped prepuce (usually left side) to identify the caudal linea alba.
Abdominal wall incision
The abdominal wall is composed of 4 pairs of abdominal muscles. Aponeurosis* from each form the linea alba.
From exterior to interior, they are:
- external abdominal oblique (fibers run caudoventrally)
- internal abdominal oblique (fibers run cranioventrally)
- rectus abdominis (fibers run parallel to the linea alba)
- surrounded by fibrous sheath made up of aponeuroses from other abdominal muscles
- components of external and internal rectus sheath vary with location
- transversus abdominis (fibers run transverse to linea)
- linea alba
- thick, white fibrous area along ventral midline
- can palpate as depressed area between paired rectus abdominis muscles
- only 2-3 mm wide in dogs, but wider and more transparent in cats
- thickest and easiest to see at the umbilicus
- thinner and harder to identify near pubis
The layer of the abdominal wall that holds sutures is the external rectus sheath.
- must be included in each suture to avoid dehiscence
The rectus abdominis is surrounded by an external and internal rectus sheath. These are made up of aponeurosesof other abdominal wall muscles. The make up of these sheaths depends on location.
|
|
Cranial to umbilicus | Caudal to umbilicus | Near the Pubis |
| External rectus sheath |
|
|
|
|
|
External Abdominal Oblique
|
External Abdominal Oblique
|
External Abdominal Oblique
|
|
|
Internal Abdominal Oblique (external leaf) | Internal Abdominal Oblique | Internal Abdominal Oblique |
|
|
|
|
Transversus Abdominis |
| Internal rectus sheath |
|
|
|
|
|
Internal Abdominal Oblique (internal leaf) |
|
|
|
|
Transversus Abdominis | Transversus Abdominis |
|
|
|
Transverse fascia | Transverse fascia | Transverse fascia |
Abdominal wall incision
Surgical anatomy
The abdominal wall is composed of 4 pairs of abdominal muscles. Aponeurosis* from each form the linea alba.
From exterior to interior, they are:
- external abdominal oblique (fibers run caudoventrally)
- internal abdominal oblique (fibers run cranioventrally)
- rectus abdominis (fibers run parallel to the linea alba)
- surrounded by fibrous sheath made up of aponeuroses from other abdominal muscles
- components of external and internal rectus sheath vary with location
- transversus abdominis (fibers run transverse to linea)
- linea alba
- thick, white fibrous area along ventral midline
- can palpate as depressed area between paired rectus abdominis muscles
- only 2-3 mm wide in dogs, but wider and more transparent in cats
- thickest and easiest to see at the umbilicus
- thinner and harder to identify near pubis
The layer of the abdominal wall that holds sutures is the external rectus sheath.
- must be included in each suture to avoid dehiscence
The rectus abdominis is surrounded by an external and internal rectus sheath. These are made up of aponeurosesof other abdominal wall muscles. The make up of these sheaths depends on location.
|
|
Cranial to umbilicus | Caudal to umbilicus | Near the Pubis |
| External rectus sheath |
|
|
|
|
|
External Abdominal Oblique
|
External Abdominal Oblique
|
External Abdominal Oblique
|
|
|
Internal Abdominal Oblique (external leaf) | Internal Abdominal Oblique | Internal Abdominal Oblique |
|
|
|
|
Transversus Abdominis |
| Internal rectus sheath |
|
|
|
|
|
Internal Abdominal Oblique (internal leaf) |
|
|
|
|
Transversus Abdominis | Transversus Abdominis |
|
|
|
Transverse fascia | Transverse fascia | Transverse fascia |
Incising the abdominal wall
- identify linea alba at the umbilicus
- make a stab incision through linea alba
- to minimize the potential for trauma
- turn the blade’s cutting surface upwards
- elevate the linea with tissue forceps
- to minimize the potential for trauma
- check for adhesions to the planned incision site by inserting forceps or a finger along proposed incision site
Incision is extended cranially and caudally using one of following techniques:
- Tissue scissors
- Scalpel blade
- Falciform fat can make it difficult to examine the cranial abdomen. It can be removed to improve visualization and facilitate closure.
Extending the abdominal wall incision using scissors
- insert tips of scissors into the stab incision
- to protect abdominal contents, elevate the scissors slightly and keep tips close to abdominal wall
- use push cutting technique to slide scissors along linea alba
- use scissor cutting technique if scissors do not slide easily
- it is common to incise just lateral to linea alba. If noticed, this can be adjusted as incision is extended
- extend the incision caudally by curving your hand backwards or using a backhand grip
Extending the abdominal wall incision using the scalpel
- insert the tissue forceps into the stab incision
- to protect abdominal contents, elevate the forceps slightly and keeping tips along the abdominal wall
- use slide cutting technique to incise the linea alba advancing the forceps as you progress
Removing the falciform fat
- removed to improve visualization of the cranial abdomen and facilitate closure
- thin fascia gently separated where connects to abdominal wall and xiphoid
- vessels in cranial region near xiphoid are clamped or ligated as necessary